WHAT is Chronic Otitis Media (COM)?
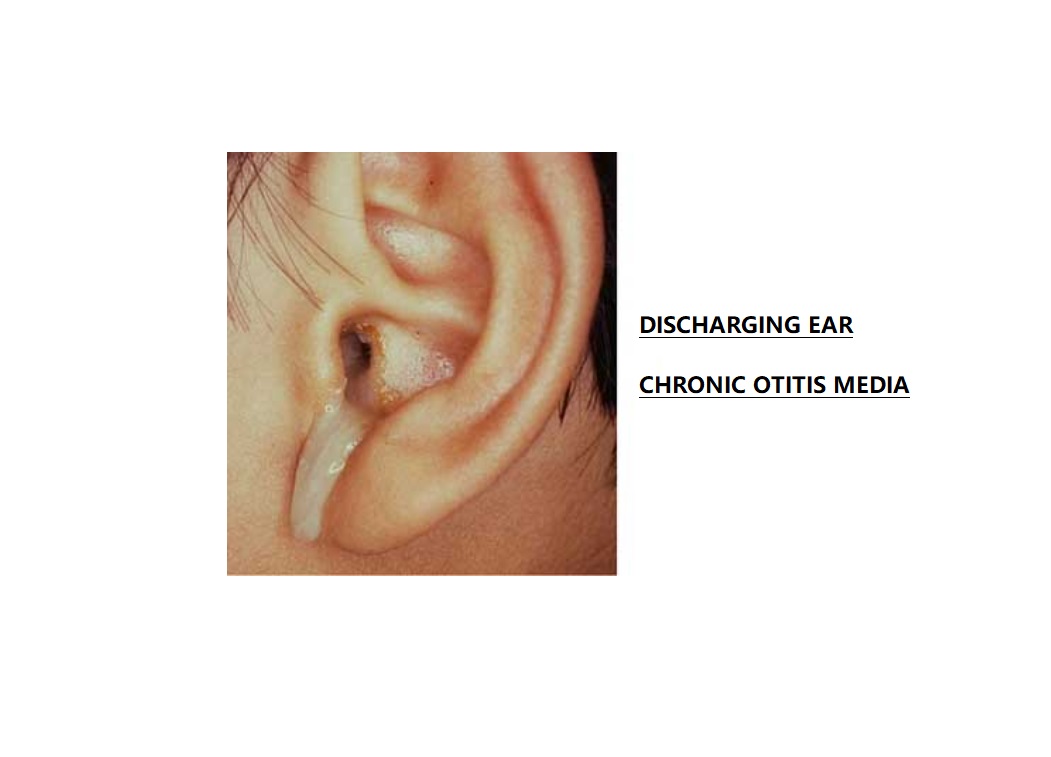
Chronic otitis media is a condition that is characterized by a long-standing middle ear infection and is associated with ear discharge and permanent hole or perforation of the tympanic membrane (eardrum).
The perforation is permanent in the case of chronic suppurative otitis media (CSOM) because the edges of the perforation are covered by squamous epithelium which prevents the natural closure of the perforation in the tympanic membrane.
The defect in the tympanic membrane (eardrum) could be in the form of —
- Retraction Pockets,
- Atelectasis, or
- Perforation.
The condition is chronic suppurative otitis media when COM presents with persistent otorrhea. So, when COM is associated with persistent otorrhea it is called CSOM.
What is CSOM?
So, CSOM stands for Chronic Suppurative Otitis Media. Let’s see the meaning of each word.
Chronic Ear infection which is present for more than 6 weeks
Suppurative Pus producing
Otitis Inflammation of the ear
Media Middle ear
So inflammation of the middle ear, which is pus producing and which is present with a long history is known as CSOM.
This is a long-standing infection of the middle ear cleft, which is marked by —
- Ear discharge and
- Permanent perforation of the tympanic membrane (eardrum).
Symptoms of Chronic Otitis Media:
The following are the most common symptoms of COM:
- Fluid draining from ear(s) or EAR DISCHARGE
- Loss of balance
- Hearing difficulties
- Ear pain
- Tugging or pulling at one or both ears
- Fever, especially in infants and younger children
CAUSES OF CHRONIC OTITIS MEDIA:
Chronic otitis media is caused by the repeated infection of the middle ear cleft.
So, the most common causes of COM are both aerobic and anaerobic bacteria are involved.
Most Common Aerobic Bacteria:
- Pseudomonas aeruginosa.
- Proteus species.
- Staphylococcus aureus.
- E. coli (Escherichia coli).
- Klebsiella species.
Anaerobic Bacteria:
- Bacteroides.
- Anaerobic Streptococci.
DIAGNOSES OF CHRONIC OTITIS MEDIA:
1) Otoscopic examination:
After history taking, an Otoscopic examination will be done.
This examination will tell us about the —
- type of perforation,
- location of the perforation,
- knowledge about the margins of the perforation,
- size of the perforation, and also
- about the middle ear mucosa.
2) Microscopic examination:
This examination must be done in all the cases.
The additional information we get by microscopic examination is about —-
- the status of the ossicular chain whether there are any tympanosclerotic foci around the ossicular chain,
- ossicular chain destruction.
- granulation tissue, adhesions in middle ear mucosa or
- any mucosal polyps.
3) Microbiology:
If there is any ear discharge, the sample should always be sent for culture and sensitivity of ear discharge.
4) Examination of the nose, paranasal sinuses, and oral cavity:
Whenever a patient is presenting with chronic otitis media these areas should also be examined to rule out —-
- tonsillitis,
- enlarged adenoid or adenoiditis, and
- sinusitis.
5) Audiological tests:
The first basic test we have to do is the tuning fork test, which helps to know about the type of hearing loss or sometimes the degree of hearing loss.
Next Pure tone audiometry (PTA) is done.
6) Radiological tests:
The most common Radiological tests advised in cases of persistent discharging ear disease are either a Both ears X-ray known as X-ray Mastoids (Schuller’s view) or an HRCT scan of both Temporal bones.
In patients with nasal symptoms, oral symptoms, and other associated clinical features, the other x-rays which may be advised is an X-ray or CT scan of the paranasal sinuses and adenoids.
Classification of Chronic Otitis Media:
COM is classified based on the presence or absence of cholesteatoma.
So, there are 2 types:
1) COM without cholesteatoma:
It is also called a TUBOTYMPANIC type of disease.
The reason why it is known as tubotympanic disease is that it involves the part of the middle ear cleft adjacent to the Eustachian tube and the mesotympanum (means middle ear cavity).
In this disease, the mucosal factor plays a role.
The inflammatory changes are confined within the middle ear and mastoid.
It is the SAFE or BENIGN because tubotympanic type CSOM is usually not associated with much of complications.
The perforation in the tympanic membrane is usually CENTRAL PERFORATION.
Central perforation means that the perforation has a tympanic membrane remnant all around it.
It is not associated with much of complications.
2) COM with cholesteatoma:
In this disease, the main factor which is playing the role is the CHOLESTEATOMA and this is responsible for all the erosions of the bone.
Cholesteatoma is a bone-eating / eroding disease.
It is called ATTICOANTRAL disease as it involves the attic region and the mastoid antrum.
Out of these two diseases, atticoantral disease due to the association with the cholesteatoma, it is associated mostly with the complications and it is considered to be a UNSAFE type of CSOM.
RISK FACTORS FOR CHRONIC OTITIS MEDIA:
1. History of recurrent acute otitis media
It is seen that in a few of the cases of acute otitis media which fail to resolve, they lead to the development of chronic otitis media as sequelae.
2. Ascending infections via Eustachian tube:
The infection can travel from certain areas like tonsils, adenoids, and infected sinuses and reach the middle ear through the Eustachian tube.
3. Allergy
4. Overcrowding
Those children who spend most of their time in crowded daycare settings are more prone to develop COM.
Because of the overcrowding what happens is that there is cross-infection in these groups of patients and they are at more risk of developing chronic otitis media (COM).
5. Poor socio-economic status
It is seen that patients belonging to poor socioeconomic status are more prone to develop COM.
COM WITHOUT CHOLESTEATOMA:
As we have seen the risk factors for developing chronic otitis media, so due to the recurrent infection whether the infection is ascending through the Eustachian tube or whether it is the sequelae of the acute otitis media, whatever the reason may be, it leads to the inflammatory changes in the middle ear and the mastoid.
As a result of which, there is a disruption of aeration of the middle ear cleft due to oedema and due to the granulation tissue.
The middle ear cleft is divided into several compartments by the mucosal folds and these different mucosal compartments get aeration through the antrum. When there will be inflammatory changes within this middle ear cleft, due to the edema and granulation tissue, it can lead to chronic otomastoiditis and certain pathological findings.
So, the pathological findings in chronic otitis media with cholesteatoma are —
- Granulation tissue in the middle ear cleft,
- Perforation of the pars tensa part of the tympanic membrane.
- Ossicular chain changes
- Tympanosclerosis.
Tympanosclerosis is a chalk-like deposit that may be seen over the tympanic membrane or around the ossicular chain. So, whenever the tympanosclerotic patches are present around the ossicular chain, they may interfere in the conduction of the sounds and it can lead to a greater degree of hearing loss in particular patients.
Types of perforation in COM without cholesteatoma:
Perforations are usually classified as per the location.
It is seen that in cases of COM without cholesteatoma, marginal perforations are the riskier type of perforation and they are often associated with complications.
So, when we (physicians) do the otoscopic examination of the patients, we have to know —
- the location of the perforation,
- the status of the tympanic annulus, and
- any sort of bony erosion.
The types of perforation are as follows —
- Anterior perforation: Anterior to handle of malleus.
- Posterior perforation: Posterior to handle of malleus.
- Inferior perforation: Inferior to handle of malleus.
- Subtotal perforation: Very large perforation of pars tensa with the intact annulus.
- Marginal perforation: Perforation with the destruction of the annulus and reaches sulcus tympanicus.
Variants of COM without cholesteatoma:
- Permanent perforation syndrome.
- Persistent mucosal disease.
These two variants are identified clinically based on the otoscopic examination and based on the history of the patients.
1. PERMANENT PERFORATION SYNDROME:
In this permanent perforation syndrome, the defect will be seen in the pars tensa of the tympanic membrane.
When the ear is dry, when there is no infection, in those cases, the mucous membrane of the medial tympanic wall appears pale pink or grey in colour.
There will not be any granulation tissue or keratinisation. Tympanosclerosis may be visible.
CLINICAL PRESENTATION:
- History of on and off ear discharge for long duration.
- Hearing loss:
- The conductive type of loss.
- Mixed hearing loss in repeated infections.
The degree of hearing loss also tells us about the status of the disease. Hearing loss between 25 to 40 dB suggests that the patient’s ossicular chain system is intact.
Whenever the hearing loss is more than 45 dB, it suggests that there might be the presence of additional lesions like tympanosclerosis, which can lead to ossicular fixation.
Hearing loss of more than 60 dB, means that there is some disruption of the ossicular chain, which usually happens due to the destruction of the long process of incus, due to inflammatory changes, and due to the presence of granulation tissue in the chronic otitis media without cholesteatoma.
2. PERSISTENT MUCOSAL DISEASE:
It is the second variant of chronic otitis media. In persistent mucosal disease, the mucous membrane is always active which means the mucous membrane of the whole middle ear cleft is involved to a greater and lesser extent. It is edematous, it is inflamed and the ear is always discharging.
The persistent mucosal disease has again 3 subtypes.
1. Tubal type:
When the perforation is seen in the anterior part with profused mucopurulent discharge. It suggests a chronic infection of the Eustachian tube.
So, whenever we get discharging ear with the perforation in the anterior part of the tympanic membrane, we have to look for the disease in the adenoids, which suggests that the infection is getting transmitted up through the Eustachian tube.
2. Tympanic type:
There will be a large defect of the pars tensa with retraction of the handle of the malleus.
The history will be of either persistent discharge or recurrent otitis media.
3. Tympano-mastoid type:
In this type, mastoid air cells are also involved. So, there is a chance of developing acquired cholesteatoma.
This group of patients does not respond to the aural toilet. Tympano-mastoid type may need cortical mastoidectomy.
AIM OF TREATMENT
- In cases of chronic otitis media, the main aim of treatment is to control the infection and to produce a dry ear because until and unless the ear is not dry, it cannot be taken up for surgery.
- The next aim of treatment is to improve the hearing by doing the surgery either at the same sitting or at a later stage once the ear is dry.
MEDICAL MANAGEMENT
- It aims to eradicate infection and it helps to produce the dry ear.
- A different way of creating a dry ear is an aural toilet. Aural toileting means clearing the ear discharge and it can be done either by dry mopping with the cotton swabs or by suction cleaning under the microscopic visualization.
- After aural toileting, topical antibiotics are advised as per the culture sensitivity report to take care of the local infection.
- Systemic antibiotics do not have that much role, but many a time it is needed in acute exacerbation of the disease.
- The patient is advised to follow certain precautions, like avoiding swimming and avoiding the entry of water into the ear while bathing or drenching in the rain.
SURGICAL MANAGEMENT
There is a great role of surgery in chronic otitis media. The main aim is to augment hearing loss.
Tympanoplasty:
It is the closure of the tympanic membrane defect. There are different methods of doing tympanoplasty by using different grafts.
The advantage of doing tympanoplasty is that it restores hearing, it prevents recurrent infections and complications like tympanosclerosis and the development of cochlear loss.
Cortical mastoidectomy:
In a few the cases, especially in the tympanomastoid type of disease where there is the involvement of the mastoid air cells, in cases of the chronic ear discharge not responding to the conservative medical management, in those cases, cortical mastoidectomy is advised.
Tympanomastoid surgery:
The goal of tympanomastoid surgery is aeration of the middle ear and mastoid, removal of irreversible diseased tissue, closure of the defect, and reconstruction of the tympano ossicular system.
Adenotonsillectomy:
In patients with adenotonsillar hypertrophy or adenoiditis, or recurrent tonsillitis, which is a source of ascending infection to the ear, in those cases, they must undergo adenotonsillectomy and it is indicated in children with persistent mucosal disease mainly of tubal variety.
SEPTOPLASTY
It is done for Deviated nasal septum
Endoscopic Sinus Surgery (ESS)
- Done for chronic rhinosinusitis.
THANK YOU
MEDICAL ADVICE DISCLAIMER:
This blog including information, content, references, and opinions is for informational purposes only.
The Author does not provide any medical advice on this platform.
Viewing, accessing, or reading this blog does not establish any doctor-patient relationship.
The information provided in this blog does not replace the services and opinions of a qualified medical professional who examines you and then prescribes medicines.
And if you have any questions of medical nature, please refer to your doctor or the qualified medical personnel for evaluation and management at a clinic/hospital near you.
The content provided in this blog represents the Author’s own interpretation of research articles.