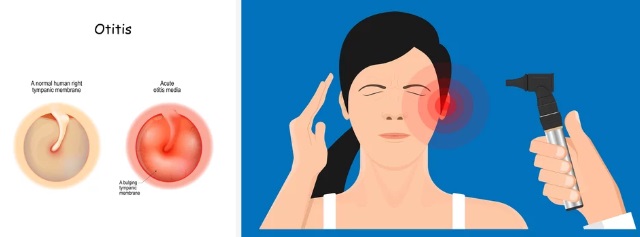
Definition
Acute otitis media (AOM) implies an acute inflammation of the middle ear cleft.
Middle ear cleft means it includes —-
- EutachianTube,
- Middle ear,
- Attic,
- Aditus,
- Antrum, and
- Mastoid air cells.
Though AOM can occur in all ages, it is mainly the disease of children as the ET is shorter, wider, and more horizontal and opens at the lower level in children. Both ears may be involved.
Etiopathology
Routes of Infection:
1) Eustachian tube:
The infection in the middle ear usually reaches through the ET.
Reflux from the nasopharynx into the middle ear occurs during the swallowing, nose blowing, and closed-nose swallowing (Toynbee’s maneuver).
It is the result of negative middle ear pressure (sniffing).
The following conditions may be present in cases of AOM:
Anatomical obstruction due to Large Adenoids and Nasopharyngeal tumors.
Currently, it is believed that it is not the obstruction but the bacterial entry into the middle ear due to the failure of protection (abnormally patent tube), which is more important.
Big adenoids, which are elevated during swallowing, may obstruct the posterior choanae and increase nasopharyngeal pressure that results in reflux.
2) Infections:
Adenoiditis, tonsillitis, rhinitis, sinusitis, pharyngitis.
Adenoids serve as a bacterial reservoir in the nasopharynx in children with AOM.
3) Forceful blowing of the nose:
The forcible blowing of the nose can push the infection into the middle ear through the ET.
4) Swimming:
Especially during diving, water enters the nose under pressure. If water is infected it can spread the infection to the nose, sinuses, and the middle ear.
5) Iatrogenic:
Postnasal packing and after adenoidectomy.
6) Feeding bottle:
In the supine position, bottle feeding may lead milk to enter middle ear via ET.
7) Pre-existing tympanic membrane perforation:
Trauma while cleaning the external auditory canal (EAC), an open hand slap on the ear, and past chronic suppurative otitis media (CSOM).
8) Fracture of the temporal bone:
In cases of head injury, the middle ear may be involved with the fracture of the temporal bone.
9) Blood-borne infection:
Rare.
Predisposing Factors
1) Reduced immunity:
Malnourishment, poor dietary habits, too much physical and mental exertion, and exposure to extremes of climate and temperatures can affect the overall resistance of the persons, and infections can occur easily.
2) Barotrauma:
Atmospheric pressure changes, especially during flying and deep-water diving, can affect ET.
3) Exanthematous fevers:
Measles, diphtheria, whooping cough.
4) Palatal disorders:
Cleft palate and palatal palsy.
5) Nasal allergy
6) Inhalants and foods
Causative Microorganisms:
Generally, viral nasal infection precedes the ear bacterial infection.
Most common are: Streptococcus pneumoniae, Haemophilus influenzae, Branhamella catarrhalis (Morexella catarrhalis).
Other common: Streptococcus pyogenes, Staphylococcus aureus.
Uncommon: Gram-negative bacilli from the skin (after trauma) such as Bacillus proteus, Bacillus pyocyneous, and Bacillus coli.
In some cases no organisms are found.
Clinical Features Pathology and Clinical Features (5 Stages)
The course of the disease is usually divided into 5 stages.
If the proper antibiotic therapy is started early during the course of AOM, the disease process may revert back from any stage.
The resolution may start even without the rupture of TM.
Most of the children will have a preceding history (cold and cough) of upper respiratory tract infection.
Infants become fussy, sleep poorly, and often pull or tug at the affected ear, and fever heralds the onset of AOM.
I. Stage of tubal occlusion:
The edema and hyperemia of the nasopharynx and Eustachian tube occlude ET, which leads to the absorption of air and the creation of negative middle ear pressure.
Symptoms:
Mild deafness.
Ear fullness and ear pain.
No fever.
II. Stage of presuppuration:
Prolonged tubal occlusion facilitates the invasion of pyogenic organisms into the middle ear and results in mucosal hyperemia. Inflammatory exudates appear in the middle ear.
Symptoms:
Marked throbbing ear pain, which can wake the child from sleep at night.
A high degree of fever and restlessness.
Bubbling sound in the ear.
Deafness though present, does not get the child’s attention due to the severe ear pain.
III. Stage of suppuration:
There occurs the formation of pus in the middle ear and somewhat in mastoid air cells. The tympanic membrane starts bulging.
Symptoms:
Excruciating ear pain.
Increasing deafness.
Constitutional symptoms due to the absorption of toxins include rising fever, which may be accompanied by vomiting, diarrhea, and even convulsions.
IV. Stage of resolution:
The TM ruptures (due to pressure necrosis) and results in otorrhea and subsidence of other symptoms. The inflammatory process begins resolving.
Symptoms:
Otorrhea: Blood tinged ear discharge (serosanguinous) later becomes mucopurulent.
Ear pain and fever subside.
V. Stage of complication:
In majority of the children, AOM is self-limiting and responds well to medical treatment. If the virulence of the organism is high and resistance of the child is poor, the infection may spread beyond the middle ear space.
Complications of AOM occur in the second week, and constitutional and infectious signs and symptoms reappear.
Diagnosis of AOM:
Acute otitis media is a clinical diagnosis.
1) Tests for hearing like Pure tone Audiometry:
They show conductive hearing loss.
2) HRCT scan of the temporal bone:
It is indicated only in cases of refractory mastoiditis.
The clouding of air cells (because of exudates) and their pressure necrosis (coalescent mastoiditis) may be seen.
Demineralization of the air cell septa is the key radiographic sign of mastoid osteitis.
3) Bacteriological examination:
The ear discharge is submitted for the culture and sensitivity to know the type of causative microorganism and the antibiotic to which they are sensitive.
Differential Diagnoses:
Otitis externa, myringitis, and bullous myringitis.
Treatment of AOM:
Medical Treatment:
There has been considerable debate on the usefulness of antibiotics for the treatment of AOM.
There are no pieces of evidence that show that antihistamines, decongestants, or any other form of adjunct medical therapy results in shortening the course of AOM.
a) Antibiotics:
Traditionally antibiotic therapy is continued till TM and hearing become normal.
b) Decongestants:
Topical ephedrine (1% in adults and 0.5% in children), oxymetazoline (Nasivion) and xylometazoline (Otrivin) nasal drops, and oral pseudoephedrine 30 mg and phenylephrine hydrochloride with or without antihistaminic is said to relieve Eustachian Tube edema and promote ventilation of middle ear.
c) Analgesics and antipyretics:
Paracetamol or Ibuprofen can take care of pain and fever.
d) Ear drop and aural toilet:
Ear discharge must be cleaned.
Quinolone/steroids ear wick/drops take care of local infection and inflammation.
e) Water is prevented from entering the ear.
f) Dry local heat:
It relieves pain.
Surgical Treatment:
1) Tympanocentesis:
It is the needle aspiration of fluid from the middle ear, and it is sent for culture and sensitivity.
The culture and sensitivity of ear fluid for knowing the organism and selecting the antibiotics is indicated in the following conditions —-
- Premature newborns
- Immunocompromised patients.
- Failure of previous antibiotic therapy
- Intracranial complications
2) Myringotomy:
An incision is put in the TM to evacuate the middle ear fluid.
The indications are following —
- Bulging eardrum
- Acute excruciating pain
- Unresponsive to antibiotics
- Facial palsy
- Intracranial complications
3) Mastoidectomy:
Diagnosis of osteitis on CT warrants mastoidectomy to remove the necrotic and infected bone.
4) Incision and drainage of Subperiosteal postauricular abscess.
5) Tympanoplasty:
In cases of permanent tympanic perforation and ossicular necrosis.
THANK YOU
MEDICAL ADVICE DISCLAIMER:
This blog including information, content, references, and opinions is for informational purposes only.
The Author does not provide any medical advice on this platform.
Viewing, accessing, or reading this blog does not establish any doctor-patient relationship.
The information provided in this blog does not replace the services and opinions of a qualified medical professional who examines you and then prescribes medicines.
And if you have any questions of medical nature, please refer to your doctor or the qualified medical personnel for evaluation and management at a clinic/hospital near you.
The content provided in this blog represents the Author’s own interpretation of research articles.