
GRANULAR MYRINGITIS
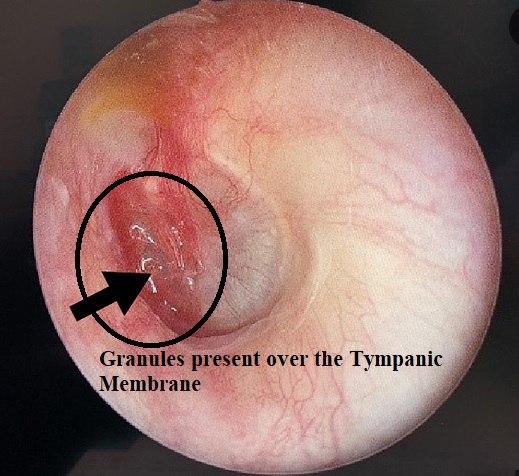
- An idiopathic inflammatory process of the Tympanic Membrane.
- Patches of granulation tissue and musicalized epithelium on the Tympanic membrane.
- In an advanced case, the complete TM gets thickened.
- Granulation tissue exudes thin transudate and may become secondarily infected.
- Secondary granulations may be associated with impacted wax, long-standing foreign body (such as a myringotomy tube), or external ear infection.
MALIGNANT or NECROTIZING OTITIS EXTERNA (MOE)
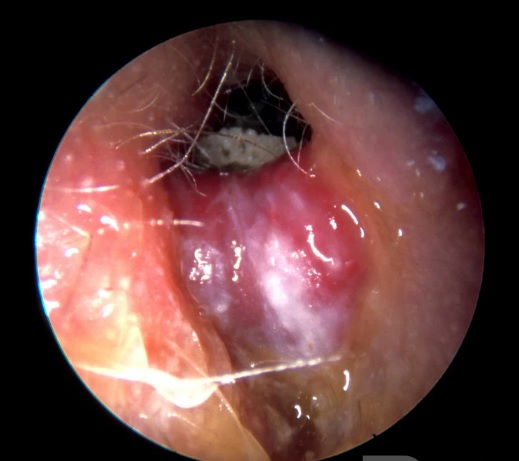
This rare Otitis Externa of immunocompromised patients is an aggressive and potentially fatal infection, which progressively spreads to the skull base and intracranial structures.
– Causative microorganisms OF MOE–
Pseudomonas aeruginosa is the most common.
Staphylococcus aureus and Staphylococcus epidermidis are rare.
– Immunocompromised patients —
Elderly diabetics, HIV/AIDS, myeloid malignancies, anti-cancerous drugs, and organ transplant recipients.
– Clinical Features of Malignant Otitis Externa (MOE) –
- Severe otalgia and otorrhea.
- Hallmark finding: Granulations in the floor of EAC at the bony-cartilaginous junction.
- The facial nerve is the most commonly involved cranial nerve.
- Advanced stage: IX, X, and XI CN palsy.
- Intracranial spread: Headache, fever, neck stiffness, and altered levels of consciousness.
- Spread of infection to the neighbouring structures: Such as the temporomandibular joint, mastoid, middle ear, and petrous bone.
- Children: Acute onset of painful otorrhea in children with immunosuppression, diabetes, or Stevens-Johnson syndrome and poor general health.
The prognosis is better than the adult form of the disease.
Investigations of MOE
- Bacterial and fungal culture
- High-resolution computed tomography (HRCT) scan
- Single-photon emission tomography (SPECT) with radionuclide tracers
Treatment of MOE
The success of aggressive medical treatment will predict the prognosis.
a) Antipseudomonal antibiotics:
Parenteral CIPROFLOXACIN (depending upon the severity) or Ciprofloxacin 750 mg orally twice a day for 6–8 weeks or longer.
In ciprofloxacin resistance cases other antibiotics such as tobramycin, ticarcillin, and third-generation cephalosporins may be used.
b) Hyperbaric oxygen therapy.
The treatment of the cause of immunosuppression, such as diabetes and HIV/AIDS.
c) Surgical debridement
of nonviable sequestration of bone is required when bone involvement is resistant to antibiotic therapy.
TYMPANOSCLEROSIS
This hyalinization and later calcification in the fibrous layer of TM appears as chalky white plaque.
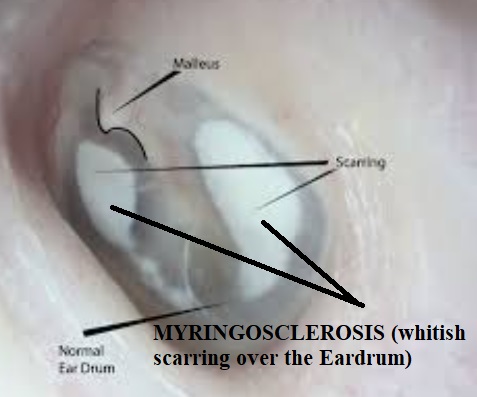
– Causes OF Tympanosclerosis:
Generally, it is the result of safe chronic suppurative otitis media (CSOM), serous otitis media, and ventilation tubes.
– Clinical features:
If the ossicles and middle ear are not involved, the condition may remain asymptomatic.
It generally affects TM. It can involve ligaments, joints of ossicles, muscle tendons, and the submucosal layer of the middle ear cleft and results in conductive hearing loss.
Traumatic Rupture of Tympanic Membrane
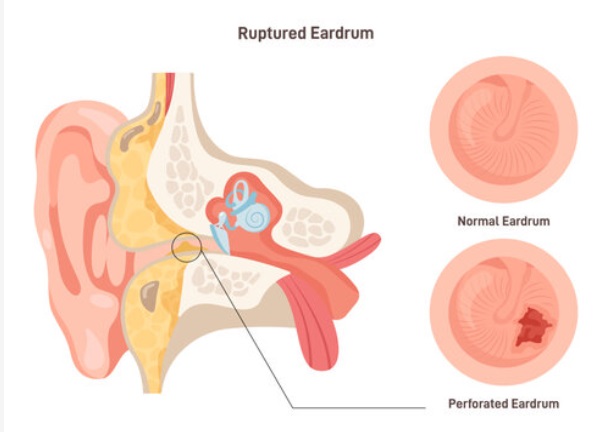
Etiology:
The injuries to the eardrum can be caused by the following:
a) Q-tip or cotton earbud injury:
Scratching the ear with hair pins, needles, matchsticks, or unskilled instrumentation.
b) Air pressure:
An open-handed slap, a kiss on the ear, a blast, and forceful Valsalva. Explosive blasts can produce more than 200 dB sound pressure level (SPL).
c) Fluid pressure:
Diving, water sports, and forceful syringing.
d) Fracture of the temporal bone.
– Clinical features
Sudden deafness, tinnitus, or dizziness after the injury.
– Ear microscopic examination:
Perforation with the edges turned either outward or inward.
– Treatment:
The edges of the perforation are repositioned and splinted under ear microscopic examination.
– Complications:
Rupture of the Eardrum may be associated with the following complications:
- Facial paralysis
- Subluxation of stapes
- Vertigo and nystagmus
- Sensorineural hearing loss
THANK YOU
MEDICAL ADVICE DISCLAIMER:
This blog including information, content, references, and opinions is for informational purposes only.
The Author does not provide any medical advice on this platform.
Viewing, accessing, or reading this blog does not establish any doctor-patient relationship.
The information provided in this blog does not replace the services and opinions of a qualified medical professional who examines you and then prescribes medicines.
And if you have any questions of medical nature, please refer to your doctor or qualified medical personnel for evaluation and management at a clinic/hospital near you.
The content provided in this blog represents the Author’s own interpretation of research articles.