
DEFINITION OF APNEA AND HYPOAPNEA
APNEA is the Absence of breathing for at least 10 seconds.
HYPOPNEA is a 30% reduction in breathing amplitude with at least 3% oxygen desaturation.
WHAT IS SLEEP APNEA?
Sleep apnea means that breathing stops for short periods during sleep.
When you stop breathing or have reduced airflow into your lungs during sleep, you don’t sleep well and you can be very tired during the day.
The oxygen levels in your blood may go down and carbon dioxide levels go up. It may also lead to other problems, such as high blood pressure, insulin resistance (or diabetes), and hyperlipidemia, as well as heart failure, pulmonary hypertension, coronary artery disease, arrhythmias, and cerebrovascular accidents.
Sleep apnea can range from mild to severe, based on how often breathing stops during sleep. For adults, breathing may stop as few as 5 times an hour (mild apnea) to 30 or more times an hour (severe apnea).
SLEEP APNEA CAN BE DANGEROUS-
Knowledge and awareness about sleep apnea are important, as it is not just snoring or the breath-holding spells that trouble a patient while sleeping, it can cause complications that can lead to even death.
A very famous Indian singer-music-composer Bappi Lahiri is known to die of complications due to OSA.

In 2016, Carrie Fisher, known for her Princess Leia role in the ‘Star Wars’ movies, passed away due to a sudden cardiac arrest. Nearly six months after, in an official statement it was revealed that Carrie Fisher’s cause of death was also due to sleep apnea and other factors which contributed to it.

CLASSIFICATION OF OBSTRUCTIVE SLEEP APNEA
The classification of Obstructive sleep apnea is done according to the AHI.
What is AHI?
The number of apnoeas and hypopnoeas averaged out per hour of sleep is regarded as the Apnoea-Hypopnoea Index (AHI).
The classification of severity of OSA has been defined as:
NO EVIDENCE of OSA: AHI < 5 apnoeas and hypopneas per hour
MILD OSA: AHI ≥ 5 and < 15 apnoeas and hypopneas per hour
MODERATE OSA: AHI ≥ 15 and < 30 apnoeas and hypopneas per hour
SEVERE OSA: AHI ≥ 30 apnoeas and hypopneas per hour.
WHAT IS OBSTRUCTIVE SLEEP APNEA?
Obstructive sleep apnea is the most common type of sleep apnea. This most often occurs because your airways are blocked or partly blocked.
This sleep disorder is caused by the relaxing of the muscles surrounding your airways as you sleep. As the muscles relax, they put pressure on or block airflow causing momentary stoppages in your breathing. This may result in loud snoring and suddenly waking up gasping for air.
Central sleep apnea is less common. It happens when the brain has trouble controlling breathing. Some people have both types and that is called complex sleep apnea.
WHAT ARE THE SYMPTOMS?
There are symptoms of obstructive sleep apnea that you may notice and symptoms that others may notice when you’re asleep.
Symptoms you may notice include:
1. Feeling extremely sleepy during the day aka EDS (Excessive Daytime Sleepiness)
2. Feeling unrefreshed or tired after a night’s sleep.
3. Problems with memory and concentration, or mood changes.
4. Morning headaches.
5. Getting up often during the night to urinate.
6. A dry mouth or sore throat in the morning.
7. Have episodes of not breathing.
8. Snore loudly.
Almost all people who have sleep apnea snore, but not all people who snore have sleep apnea.
9. Toss and turn during sleep.
10. Have nighttime choking or gasping spells.
HOW IS IT DIAGNOSED?
1) General Physical Examination
2) Endoscopy of Nose
3) Oral Cavity and Throat Examination
4) Sleep Study
5) DISE (Drug-induced Sleep Endoscopy)
General Physical Examination
Your doctor will probably do a general physical examination like measurement of weight, height, pulse rate, BP, BMI, Neck circumference, Waist circumference, etc, and ask about your past health.
It is seen that patients with OSA on examination may reveal —
– Obesity with BMI > 30 (seen in 70% of cases),
– Increased Neck circumference (often > 40 cm), and
– Increased Waist circumference (men > 94 cm; women > 80 cm).
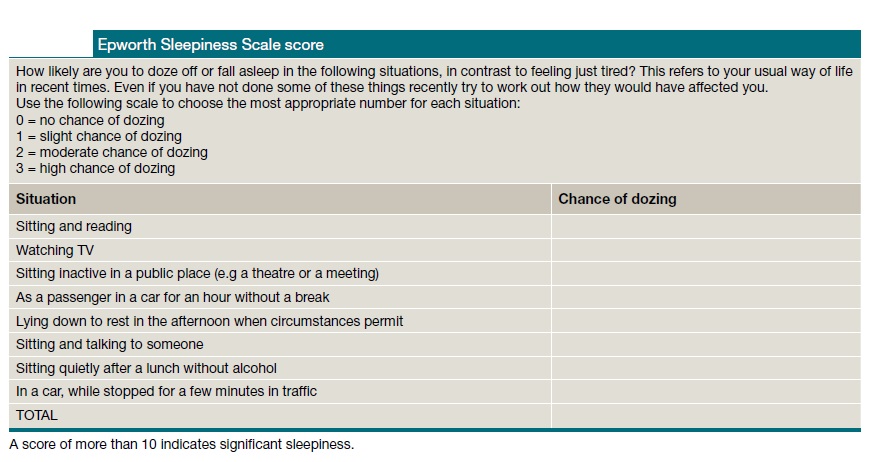
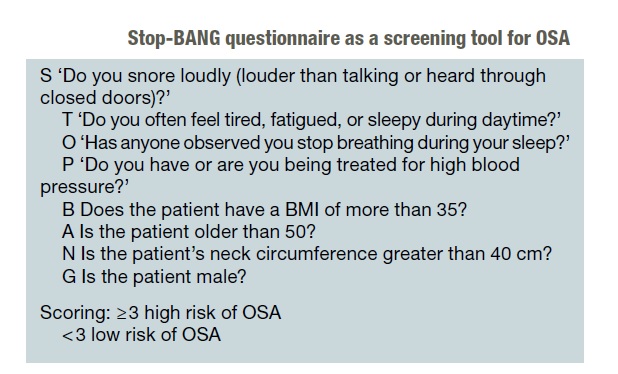
The doctor may also ask you or your bed partner about your snoring and sleep behavior and how tired you feel during the day, along with filling out an Epworth sleepiness scale and a STOP-BANG questionnaire form.
Excessive sleepiness is a subjective marker of OSA, although it can affect up to 12% of the patients and is more common in subjects with snoring, obesity, diabetes mellitus, and renal failure.
It is difficult to quantify consistently or objectively, but the Epworth Sleepiness Scale (ESS) score and STOP-BANG questionnaire are commonly used as a validated simple self-administered assessment tool for screening of OSA.
Endoscopy of Nose
This will be followed by a Nasal examination where if required an ENDOSCOPIC EXAMINATION OF NOSE will be done.
A rigid zero degree nasal endoscope will be introduced in the nasal cavities and the inside of the nose will be assessed for any —
- Deviated nasal septum,
- Hypertrophied or swollen turbinates,
- Rhinits, or
- Nasal mass like polyp etc.
Throat Examination
The oral cavity, as well as throat, will be examined and the patient will also be assessed for —
- Heavy and large tongue
- Enlarged soft palate
- Enlarged tonsils
- Swollen or Elongated uvula
- Area of Oropharyngeal airway
Sleep Study
Your doctor may suggest a sleep study.
Sleep studies are a series of tests that look at what happens to the body during sleep. They check for how often you stop breathing or have too little air flowing into your lungs during sleep. They also find out how much oxygen you have in your blood during sleep.
SLEEP STUDY may take place in your home or it might take place at a sleep center where you will spend the night.
If your sleep apnea doesn’t improve with treatment, you may have more tests to find out what’s causing it.
DISE (Drug-induced Sleep Endoscopy)
Sleep endoscopy, also known as sleep nasendoscopy (SNE) or drug-induced sleep endoscopy (DISE), is a very useful procedure for studying the real-time status airway in a sleeping patient with Obstructive Sleep Apnea (OSA).
The role of DISE comes due to the difficulty faced by the doctor in accurately establishing the site of obstruction in a conscious patient with a diagnosis of OSA.
Hence, using midazolam as a sedating agent under the supervision of an anesthetist, the patient is sedated and a flexible fiberoptic endoscope is passed through a sleeping patient’s nasal cavity to assess pharyngeal structures for evidence of obstruction.
Once the surgeon, the assistant with the flexible fiberoptic endoscope equipment trolley is ready, the anesthetist is signaled to start the patient with an infusion of the sedating agent. The anesthesiologist must carefully titrate the propofol infusion in order to cause obstructive apnea, but no central apnea.
When the patient can no longer be aroused by voice, the flexible endoscope is introduced into the nasal cavity.
The surgeon fully examines the nasal cavity for any deviated nasal septum, swollen turbinates, rhinitis, nasal mas, polyp, etc., and then advances into the nasopharynx. Wait in the nasopharynx until the patient begins snoring.
Examine the nasopharynx, velopharynx, and hypopharynx. Utmost attention is given to assess the degree of collapse of these structures and the following grading scale is used:
- 0-25% collapse
- 26-50% collapse
- 51-75% collapse
- 76-100% collapse
The following structures are also carefully assessed :
- If there is Obstruction at the level of the palate – Palate, tonsils, and lateral pharyngeal wall
- If there is Obstruction at the level of the hypopharynx – Base of tongue, epiglottis, and lateral pharyngeal wall
(There is one study that mentions that approximately 23% of patients had an epiglottis collapse that was NOT seen on awake endoscopy and this epiglottis collapse was the main cause of snoring in the patient.)
HOW IS IT TREATED?
(I) HOME REMEDY AND LIFESTYLE CHANGES:
Many patients use over-the-counter devices that claim to help the patients and reduce snoring. These devices are-
- Nasal srips like Breathe right etc
- Nose Clips snore stopper eg Silicone Magnetic Anti Snoring Device Nose Clip
- Antisnore Chin straps
You may be able to help treat sleep apnea by making some lifestyle changes. Hence, you could try to-
- Lose weight,
- Sleep on your side.
- Avoid alcohol and medicines like sedatives before bed.
- Elevation of the bed head
- Avoidance of sleeping on back
- Avoidance of tobacco and narcotics.
Driving should be avoided if the patient complains of excessive daytime sleepiness.
Patients with OSA must inform the relevant driving licensing authority of the diagnosis.
However, driving may be allowed if symptoms are controlled on treatment, with confirmation by medical opinion.
(II) MEDICINES
Treatment of nasal congestion using nasal steroids like Fluticasone furoate/propionate, Mometasone, etc. may be helpful, especially if there is a nasal obstruction or upper airway resistance due to rhinitis.
Evidence suggests that TRAZODONE, a commonly prescribed antidepressant with hypnotic properties, increases effectively the arousal threshold without altering upper airway muscle activity, making this medication a potentially useful candidate for treating OSA.
Modafinil is approved by the US Food and Drug Administration (FDA) for use in patients TO REDUCE residual daytime sleepiness despite optimal use of CPAP. The most improvement has been seen in patients who have taken modafinil at doses of 200-400 mg/d.
Armodafinil, the R-enantiomer of modafinil, is also now FDA approved for use in these patients.
(III) ANTI SNORING and ANTI SLEEP APNEA MACHINES
Sleep apnea is often treated with machines that deliver air through a mask to help keep your airways open.
These include:
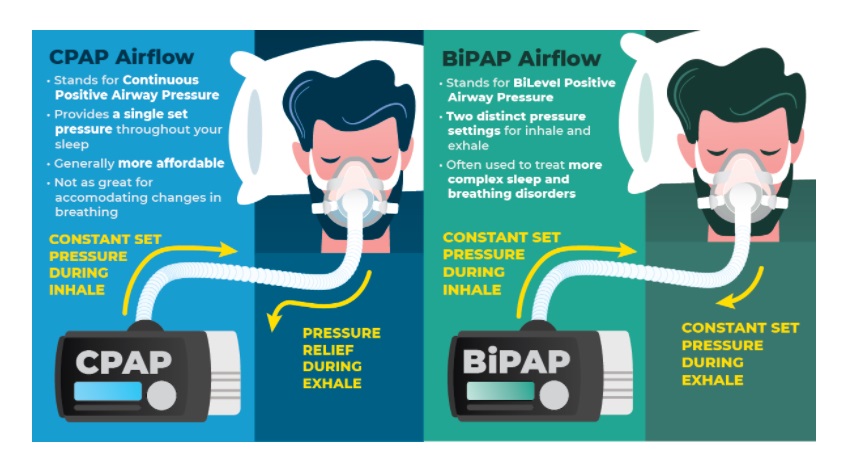
1. Continuous Positive Airway Pressure (CPAP):
Continuous positive airway pressure (CPAP) is regarded as the mainstay of OSA treatment. It is the first treatment choice and the most widely used.
CPAP is a small machine that you can use at home every night while you sleep.
When you have sleep apnea, this can help you sleep better, feel better, and avoid future health problems.
This increases air pressure in your throat. It keeps your airway open when you breathe in. The mode of action can be regarded as a ‘pneumatic splint’ whereby the air pressure generated via a tube and mask, through the nasal and/or oral passageway, prevents collapse of the pharyngeal and palatal walls in a patient with OSA is sleeping.
CPAP helps you to have more normal sleep, so you feel less sleepy and more alert during the daytime.
CPAP may help keep heart failure or other heart problems from getting worse. It may help lower your blood pressure.
If you have a bed partner, they may also sleep better when you use a CPAP. That’s because you are not snoring or restless.
Your doctor may suggest CPAP if you have:
- Moderate-to-severe sleep apnea.
- Sleep apnea and coronary artery disease (CAD).
- Sleep apnea and heart failure.
The CPAP machine will have one of the following:
- A mask that covers your nose and mouth.
- A mask that covers your nose only.
- A nasal pillow that covers only the openings of your nose.
If using CPAP is not comfortable, or if you have certain side effects, work with your doctor to fix them.
Be sure the mask, nasal mask, or nasal pillow fits well.
See if your doctor can adjust the pressure of your CPAP. If your nose or mouth is dry, set the machine to deliver warmer or wetter air or try using a humidifier.
If your nose is runny or stuffy, talk to your doctor about using a decongestant medicine or steroid nasal spray.
Read and follow all instructions advised by the doctor and written on the label of the machine.
Your doctor may also help you with problems like swallowing air, bloating, or claustrophobia.

2. Bilevel Positive Airway Pressure (BiPAP):
You may also hear this called BiPAP. This uses different air pressures when you breathe in and out.
It’s a machine that gives you air through your nose, mouth or both. It uses different pressures when you breathe in and out.
Higher pressure is used when you breathe in and lower pressure when you breathe out, for example, inspiratory positive airway pressure (IPAP) between 10 cm H2O and 20 cm H2O, and expiratory positive airway pressure (EPAP) between 5 cm H2O and 10 cm H2O.
It may have a mask that covers your nose and mouth (this may be called a full face mask) or a mask that covers only your nose. It could also have a nasal pillow that covers only the openings of your nose.
When the patient sleeping does not breathe for a programmed period of time, the BiPAP may be set to deliver a breath. This is usually set as a minimum breath that sets minimum breaths per minute (BPM). This setting is designed so that the patient breathes a set frequency of breaths per minute. BiPAP is often used when CPAP is not tolerated by the patient.
One of the many advantages of the BiPAP machine is that the strain is decreased during expiration. This limits the amount of energy expended during exhalation. It is easier to breathe out with BiPAP than with CPAP.

3. Adaptive Servo Ventilation (ASV):
It senses pauses in breathing and adjusts air pressure. It is mostly used for central sleep apnea.
It is a non-invasive option to help you breathe in a steady pattern during the night. This device tracks how you breathe while you sleep. They adjust air pressure according to your breathing pattern to help you breathe more normally during the night.
Your doctor will set the original air pressure on your ASV.
ASV is needed if you have obstructive sleep apnea, complex sleep apnea, central sleep apnea, or mixed sleep apnea. ASV is prescribed if your CPAP or BiPAP has not worked for your sleep apnea.
WHEN SURGERY IS NEEDED?
If your tonsils, nasal septum, or other tissues are blocking your airway, your doctor may suggest surgery to open the airway.
Surgical treatment may involve various procedures that are performed in different stages depending on the patient’s site of obstruction.
The most commonly performed procedures include —
- Nasal reconstruction,
- Uvulopalatopharyngoplasty (UPPP),
- Advancement genioplasty,
- Mandibular osteotomy with genioglossus advancement,
- Hyoid myotomy, and suspension,
- maxillomandibular advancement (MMA) with advancement genioplasty, etc.
An important thing to mention here is that In general, operations performed to increase airflow through the nose, such as–
- Removal of nasal polyps or turbinates, or
- straightening a deviated nasal septum,
generally, DO NOT completely cure obstructive sleep apnea (OSA) but may improve daytime and nighttime breathing through the nose and may enable better use of positive airway pressure.
UVULOPALATOPHARYNGOPLASTY (UPPP):
The most common operation performed is called UVULOPALATOPHARYNGOPLASTY (UPPP). This surgery may be used to improve obstructive sleep apnea that has not been helped by other treatments.
Obstructive sleep apnea happens when your throat is narrow or blocked by tissue. After UPPP, you may breathe more easily or even snore less. This surgery may not completely fix the problem if the tongue relaxes when you sleep and blocks the airway. So you may still need to use continuous positive airway pressure (CPAP).
You will probably go home the day after surgery. In about 1 to 2 weeks, you can probably go back to work or most of your usual activities, but you may need up to 3 to 6 weeks to fully recover. Over the next 3 to 6 weeks, you should start to have better airflow. You may find that you snore less or not at all. Each person recovers at a different pace.
RADIOFREQUENCY VOLUME REDUCTION FOR THE THROAT:
Radiofrequency volume reduction for the throat may reduce snoring.
It may also be used to treat obstructive sleep apnea.
First, your doctor will numb the area with a local anesthetic. Then, a needle is put into the roof of your mouth (palate) or your tongue. A small electric current goes through the needle. This opens up the blocked area. The area will heal over the next 6 to 8 weeks. As it heals, the flow of air should improve and you may snore less. Most people go home right after it is done. You will probably be able to return to work or your normal routine the next day. You may need more than one treatment.
MAXILLOMANDIBULAR ADVANCEMENT:
In this operation, the upper and lower jaws are surgically moved forward to enlarge the airway. This operation is substantially more complex than UPPP, with greater risk to the patient and a much longer recovery period.
TRACHEOSTOMY:
A tracheostomy is a surgically created opening in the trachea below the level of the larynx or voice box.
This bypasses the area of obstruction in OSA.
Tracheostomy is the primary treatment for severe OSA before the introduction of positive airway pressure therapy. It is used for very severe cases that cannot be treated otherwise.

Other Procedures:
Several other operations have been performed for OSA. These include–
- Hypoglossal nerve stimulation,
- Stiffening the soft palate with stents,
- Advancement of the front of the lower jaw, and
- Relocation of the hyoid bone.
These may benefit in selected cases. There are many surgical options for the treatment of sleep apnea for patients who cannot tolerate CPAP therapy. Because the airway pattern and the severity of obstruction vary between
individuals, the surgical treatment also varies to that particular individual. Often it takes a combination of procedures to achieve success.
THANK YOU
MEDICAL ADVICE DISCLAIMER:
This blog including information, content, references, and opinions is for informational purposes only.
The Author does not provide any medical advice on this platform.
Viewing, accessing, or reading this blog does not establish any doctor-patient relationship.
The information provided in this blog does not replace the services and opinions of a qualified medical professional who examines you and then prescribes medicines.
And if you have any questions of medical nature, please refer to your doctor or the qualified medical personnel for evaluation and management at a clinic/hospital near you.
The content provided in this blog represents the Author’s own interpretation of research articles.